
Abstract
Exposure therapy for anxiety and related disorders is the psychological intervention with the strongest support for its efficacy and effectiveness to date. Yet, it is the least used evidence-based intervention in routine clinical practice, with a long-acknowledged public relations problem. Despite a wealth of research aimed at improving uptake of exposure, exposure’s marketing and branding remains an untapped target. We first introduce principles from the marketing literature to propose that the field take steps toward a rebranding and repackaging of exposure therapy to support efforts to implement it widely. Second, we present preliminary data on clinician preferences for the use of alternative terminology developed to be more palatable and marketable - “Supported Approach of Feared Experiences – Cognitive Behavioral Therapy (SAFE-CBT)” - compared to traditional terminology. This initial survey indicated that most clinicians preferred use of the SAFE-CBT term when talking to patients, whereas only a minority preferred it for use among training clinicians. We conclude by discussing implications of these results for future efforts to implement exposure therapy more widely and set an agenda for future research in this space.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Up to 30% of the United States population will experience debilitating anxiety at some point in their life, with this maladaptive anxiety maintained and reinforced by avoidance of things that cause fear and anxiety (Kessler et al., 2012). Undertreated anxiety is further associated with a host of negative sequelae, including heightened risk for suicide (e.g., Machell et al., 2016; Sareen et al., 2005). Fortunately, there is strong evidence for psychosocial cognitive behavioral therapy (CBT) interventions that are also remarkably effective at reducing functional impairment (Hofmann et al., 2012). Most notably, exposure therapy (“exposure” or “exposure and response prevention”) is the key intervention strategy through which CBT improves outcomes for people with anxiety. Based on the well-validated theory that anxiety is maintained and worsened by avoiding feared stimuli, exposure involves guided therapist support for patients to gradually confront and increase their tolerance of feared stimuli (Abramowitz et al., 2019).
As many as 9 in 10 of those who seek treatment for anxiety will not receive this effective and clear first-line treatment for anxiety (Hipol & Deacon, 2013; Whiteside et al., 2016a, b). Most practicing clinicians– even those who identify as CBT practitioners– do not use exposure with their anxious patients (Becker-Haimes et al., 2017a; Chu et al., 2015). Many clinicians’ hold negative beliefs about exposure therapy, perceiving it as harmful, unethical, or intolerable, as it involves intentionally encouraging individuals to experience distress (Deacon & Farrell, 2013; Gagne et al., 2021; Olatunji et al., 2009). Clinicians instead rely on less effective, and at times contraindicated, treatments (Becker-Haimes et al., 2017a; Hipol & Deacon, 2013). For example, clinicians opt for other CBT components, such as relaxation, or they recommend strategies that promote avoidance (e.g., education or occupational accommodations). While accommodations may be appropriate in the short-term to encourage approach behavior, long-term reliance on them is associated with poor outcomes and is contrary to the goals of enhancing fear tolerance and improving functioning (Kagan et al., 2018).
The reasons why clinicians do not use exposure are complex; in addition to negative attitudes about exposure cited above, organizational support is often limited (Becker-Haimes et al., 2020). This is consistent with the broader implementation literature highlighting the importance of attending to the multiple contextual levels (e.g., organizational leadership, policy) that influence clinician practice use (e.g., Damschroder et al., 2009). However, the literature surrounding exposure implementation has generally overlooked a critical implementation target: exposure’s branding, starting with the nomenclature. In this manuscript, we propose that an effort to rebrand exposure therapy, beginning with more accurate and palatable terminology to describe it, holds potential to support efforts to increase exposure’s acceptability.
Why rebrand exposure?
Little attention has been paid to considering the mental health provider as an end-user, or consumer, of interest with regards to psychosocial treatment development (Lyon & Koerner, 2016). It is only within the past decade that treatment developers have begun to seriously consider how to optimally package treatment materials to make them easily usable and sufficiently flexible for a broad swath of the clinician population to use effectively (Chorpita et al., 2020; Lyon et al., 2020, 2021). This is an area in its infancy, especially with respect to conceptualizing health service providers as consumers (Dopp et al., 2020). Virtually no work has considered the importance of leveraging known marketing principles to support uptake of evidence-based interventions among clinicians (Proctor et al., 2021).
In the broader marketing literature, careful rebranding (i.e., changing the image of a product) has demonstrated effects on improving desired outcomes (Tsai et al., 2015). One’s brand is essential to how one is perceived to target end-users (Maurya & Mishra, 2012). Integral to any branding effort is an effective name (see Danesi, 2011 for a detailed review of naming strategies for effective branding and their importance). Names are not simple identifiers of a product; rather, they bestow meaning and identity to a product and are the backbone of any marketing effort (Danesi, 2011; Wheeler, 2003). While there are multiple approaches to developing a brand name, careful composition of a “good” name that reflects the intended meaning of the brand is critical (Aslerhan & Ashlerhan, 2012). Pharmacological companies and other commercial industries understand this. Prozac and Xanax are household words; “selective serotonin reuptake inhibitors” and “alprazolam” are not. Mental health clinicians and researchers are beginning to realize the importance of effective branding of our treatments to patients. Unsurprisingly, the names and descriptions researchers assign to therapies they develop are less enticing than those whose development was guided by marketing principles with the patient end-user in mind (Becker et al., 2020). It is thus reasonable to assume that treatment developers could benefit from naming psychosocial treatments with more weight given to market appeal; in other words, a name consistent with the image of exposure as a compassionate and effective treatment.
We must acknowledge that exposure therapy is poorly named (Deacon & Farrell, 2013). Imagine you are a clinician interested in learning how to treat anxiety disorders, which are among the most common presenting problems. What sounds more compelling, intuitive, and empathic: “relaxation strategies” or “exposure and response prevention?” If you answered, “relaxation strategies,” you are in good company. We frequently lead workshops and begin by asking clinicians, “what comes to mind when you hear the term exposure therapy?” The answers range from “scary” to “forcing people to do things they are afraid of” to “people flashing themselves.” It is ironic that the name of the best treatment we have for anxiety disorders evokes anxiety in clinicians! Clinician misperceptions of gradual exposure, which is what most experts are referencing when they discuss exposure therapy, is thus conflated with flooding, a more controversial and less empirically supported approach for managing anxiety that involves patients tackling their fears as quickly as possible.
The current “exposure” nomenclature thus evokes an identity that is inconsistent with its mission to improve the lives and well-being of those with anxiety and related disorders. Clinician concerns (and arguably, misconceptions) about exposure persist even though it has a remarkably high degree of objective market viability and appeal (Proctor et al., 2021). From a marketing perspective, exposure is a well-defined intervention with strong support for its effectiveness and a clearly defined adopter group (i.e., clinicians). It has demonstrated and significant comparative advantage with life-changing potential for both patients and their families. There is overwhelming evidence that exposure is well-tolerated by patients, is associated with few side effects, and is effective for anxiety disorders, obsessive-compulsive disorders, and post-traumatic stress disorder, with increasing support for its use in other populations such as eating disorders (Butler & Heimberg, 2020; Hofmann et al., 2012). Those who deliver exposure regularly know that it is critical to define it as a treatment that gradually supports people to face what that they are afraid of, so that fear no longer runs their life and they can engage in the activities that are most meaningful to them. When explained this way, clinicians use words like “supportive,” “helpful,” and “necessary” to describe exposure. Patients rarely decline exposure once it is properly introduced; dropout rates are no higher than they are for other psychosocial treatments (Garcia-Palacios et al., 2007; Ong et al., 2016). Despite this, few clinicians deliver exposure to their anxious patients.
To expand the reach of exposure to ensure that all those in need of anxiety treatment can receive it, it is worth exploring whether alternative terminology that more accurately reflects the reality of exposure will support improved intervention appeal to (and subsequent uptake among) clinicians. We composed the term “Supported Approach of Feared Experiences – Cognitive Behavioral Therapy (SAFE-CBT)” as a potential alternative to the terms “exposure therapy” and “exposure and response prevention” within the mental health lexicon. This term was created for several reasons. First, it is descriptive– clinicians will support patients in facing their fears – and implies treatment safety and tolerability. Although it is important for clinicians to never guarantee that a given feared (or life) experience is without any risk, SAFE-CBT is also consistent with leading theories that emphasize the importance of supporting patients to learn that they can safely engage in feared experiences via exposure (Craske et al., 2014). Second, joining the descriptor acronym (SAFE) with the more traditional CBT moniker acknowledges this treatment’s history as a cognitive behavioral strategy but also allows it to stand on its own. Third, it innately stands in opposition to some of the most common negative perceptions about the intervention reported by clinicians (i.e., that it is harmful or unethical; Olatunji et al., 2009).
A renaming effort will succeed only if the alternative name is perceived as appealing by the target consumers – in this case, practicing clinicians. Informal polling of our clinical colleagues suggested that nearly all would prefer the term SAFE-CBT when talking about exposure to patients; however, there was hesitancy about using the term among clinicians. We built on this informal polling to conduct preliminary testing of SAFE-CBT among clinicians. We hypothesized that SAFE-CBT would be considered preferable to traditional exposure terminology among clinicians for use both with training novice clinicians and with patients.
Methods
Procedures
We conducted a brief, anonymous electronic survey with 49 clinicians via Qualtrics. We contacted all registered site users of an online toolkit to support clinician use of exposure therapy (www.bravepracticeforkids.com; Becker-Haimes et al., 2017b) with valid contact information (N = 364). This sampling approach ensured we captured a target audience of clinicians at least moderately informed about exposure therapy. All potential participants were contacted by email and invited to participate in a larger survey about exposure therapy up to four times. Survey design and execution was conducted in accordance with adapted principles of the Tailored Design Method (Dillman et al., 2014). All emails contained a link that allowed potential participants to opt out of the study and future mailings. There were 15 bounce-backs and 3 individuals who opted out of survey recruitment emails; 49 individuals completed the survey (14% response rate). Data presented here were drawn from select survey items included in the larger survey that were specifically included to assess clinician perspectives about exposure terminology.
Participants
Survey respondents averaged 35 years old (SD = 8.41) and largely identified as female (75.5%). Racial identities were White (73.5%), Asian (10.2%), Black or African American (2.0%), Biracial or Multiracial (2.0%), or Hispanic (2.0%). Regarding highest degree obtained, approximately half (49.0%) were doctorate-level and 46.9% were master’s level. Most participants (67.3%) reported a professional discipline of clinical psychology, and the next most prevalent professional discipline was social work (10.2%). Most (85.7%) endorsed that they provided direct clinical services; 57.1% were licensed. Clinicians reported an average caseload of 24.5 (SD = 17), with an average of 15 patients treated per week (SD = 10). Clinicians worked in a range of professional settings; the most common were private practice (36.7%) and academic medical center/hospital settings (32.7%). Most (73.5%) reported that they had previously received formal training or supervised practice in exposure therapy.
Compliance with ethical standards
All respondents provided informed consent prior to participation and were entered into a lottery to win one of ten $35 electronic gift cards as a thank you for participating. Procedures were approved by the Institutional Review Board at the University of Pennsylvania.
Survey measures
Terminology preference
Clinicians reported on two forced choice questions about the terminology they preferred: (1) “If you were recommending a friend seek mental health treatment for anxiety, what language do you think would be most comforting when it comes to describing the treatment?,” and (2) “If you were teaching a novice clinician about evidence-based psychosocial treatments for anxiety, which terminology would you prefer to use to describe the leading evidence-based treatment models?” For each, clinicians were asked to select either (a) Exposure Therapy (ET), (b) Exposure-Based Cognitive Behavioral Therapy (EB-CBT), and (c) Supported Approach of Feared Experiences – Cognitive Behavioral Therapy (SAFE-CBT).
Clinician demographics
Clinicians also completed a background questionnaire about their demographics and clinical training background.
Results
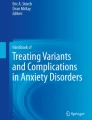
Figure 1 shows respondent preferences for each of the three terminology options for both “a friend seeking mental health treatment for anxiety” and a “novice clinician.”

Terminology preferences among percentage of respondents
Friend seeking treatment
When asked to think about preferred terminology to use with someone seeking treatment for anxiety, there was relatively equal distribution of preferences across all three categories among respondents (X2(2) = 3.98; p = .14). Consistent with informal polling of colleagues and study hypotheses, the biggest preference for terminology for someone seeking mental health treatment was SAFE-CBT, (42.6%). The remainder of participants were relatively split between the more traditional terms, with slightly more participants indicating a preference for EB-CBT (36.2%) over Exposure Therapy (21.3%).
Novice clinician
In contrast to hypotheses, although consistent with our informal polling, fewer respondents reported preference for the use of SAFE-CBT for clinicians-in-training (8.7%), as compared to those that indicated preference for EB-CBT (52.2%), closely followed by Exposure Therapy (39.1%). One way chi-square goodness of fit tests suggested these differences were statistically significant. (X2(2) = 12.67; p = .002).
Comparison between target consumers
Critically, preferences varied sharply as a function of whether respondents were asked to think about the ideal terminology for a friend seeking treatment vs. a novice clinician (X2(4) = 10.44; p = .034), with overall greater positivity for SAFE-CBT when asked to think about a friend seeking treatment compared to a novice clinician in training.
Discussion
The term “exposure therapy” sounds antithetical to the guided therapist support upon which this treatment relies. Studying how to rebrand exposure is an area ripe for additional work and research. First and foremost, involving stakeholders in the branding process has been proposed as an important step for the ultimate success of a branding effort (Voyer et al., 2017). In this initial, preliminary study, we surveyed practicing clinicians informed about exposure therapy about their perception of a proposal for an exposure rebrand (SAFE-CBT) compared to traditional nomenclature. Contrary to study hypotheses, SAFE-CBT was not unanimously perceived as a welcomed alternative to traditional nomenclature for use with clinicians. However, it is noteworthy that there was a stark and statistically significant difference between the language clinicians reported wanting to use to explain the treatment to friends seeking care, compared to that used for clinicians in training. While further qualitative work is needed to understand this discrepancy in language preferences for friends versus novice colleagues among clinicians experienced with exposure therapy, this may indicate a different valence or meaning behind SAFE-CBT compared to exposure therapy that might make it more palatable or attractive.
Findings provide proof of concept that further exploring the potential benefit of a rebrand of exposure is warranted. This initial pattern of results also suggests that any rebranding effort may need to concomitantly plan to classify exposure therapy as a technical term that should be retained in the literature. For example, even though sertraline is branded as Zoloft, prescribing physicians often rely on or use the technical term sertraline in their training. Careful consideration of how and when the term exposure should be retained within the context of a rebranding effort will be an important step for future research. That said, it is important to note that a rebrand will not do all the work to change clinician negative clinician beliefs about exposure and increase clinician exposure use; continued work designing tailored implementation strategies across contextual levels will be critical. However, a rebrand may make this work easier by reducing misperceptions about this therapy on the part of clinicians and patients alike. This is critical, as most exposure implementation efforts directly target clinician negative beliefs about exposure, with mixed success (Trivasse et al., 2020).
These initial data on SAFE-CBT are preliminary and have limitations worth noting. SAFE-CBT represents only a single potential alternative for a revised brand name for exposure and we included only a single stakeholder group (practicing clinicians) who were already moderately informed about exposure therapy. To fully evaluate the potential for a rebranding effort to have substantial impact, future work in this space should be conducted: (1) with more rebranding terminology options, and (2) in partnership with stakeholders from a diversity of backgrounds and experiences reflective of the target end-user of exposure therapy, including graduate students and novice clinicians across mental health disciplines (e.g., psychology, social work, counseling), practicing clinicians from a range of settings (e.g., private practice, academic medical centers, community mental health, integrated primary care), training directors, researchers, and other leaders in the mental health space. Although not a focus in this early work, it is critical that individuals with anxiety disorders are actively included in this process to optimize the likelihood that the selected brand name holds optimal appeal to clinicians and patients alike.
We also note several methodological limitations of data collected. Our survey response rate was relatively low (14%), although not atypical for online surveys (Sammut et al., 2021). It is also important to note that our survey was sent out during the COVID-19 pandemic. This also may have lowered our response rate and it is possible that clinicians experiencing higher pandemic-associated distress were less likely to participate in this survey. Most importantly, our sample, while intentionally selected for its familiarity with and interest in exposure, is not generalizable to the broader population of practicing mental health clinicians. The clinical background of survey respondents was largely clinical psychology, doctoral level, and relatively savvy with exposure; this contrasts with the largely master’s level mental health workforce (Hoge et al., 2019). Data on rebranding in the broader literature suggests that an individual’s perceived loyalty towards a brand may moderate the extent to which they approve of a rebrand (Hatch & Schultz, 2003; Williams et al., 2021); in other words, those most loyal to an original brand may be most resistant to change. As noted above, it will be particularly critical to survey novice clinicians and those from other disciplines on their preferences and likelihood of using a treatment branded with the SAFE-CBT moniker over more traditional terminology.
Conclusions and future directions
Exposure strategies originated 100 years ago and have been the subject of hundreds of clinical trials. Many clinicians and researchers dedicate their whole careers to delivering or advancing the clinical efficacy of exposure strategies for those suffering from anxiety and related disorders. Determining if and how to make a small, but fundamental, shift in language to rebrand exposure will not be easy and likely will require a multitude of strategies. Formative work, as mentioned above, should focus on further testing SAFE-CBT, along with other alternative terminology, with many different stakeholders. Additional work might include testing the impact of coordinated social media campaigns and collaboration with leading psychiatric organizations. Future work in this space might also explore partnering with experts in market research and communications, along with leaders of scientific organizations (e.g., the Anxiety and Depression Association of America), foundations (e.g., the International Obsessive Compulsive Disorder Foundation), and leading academic clinicians, researchers, and teachers. Testing different marketing strategies with a revised name and their impact on clinician perceptions of exposure may also prove a fruitful area of research with implications for how to optimize marketing of other interventions that suffer from research to practice gaps. Rebranding is also not without risk (e.g., Haig, 2003). Any effort to study the impact of a rebrand must be accompanied with careful assessment of any unwanted or unanticipated effects.
Of note, we focused here on rebranding and renaming a treatment to reduce clinician aversion to adopting an effective treatment. While beyond the scope of this paper, we think it is important to comment that a public (i.e., patient-facing) education campaign on the effectiveness of psychosocial treatments (i.e., SAFE-CBT or another chosen name) for anxiety disorders is long overdue, especially given our findings that SAFE-CBT was more preferred for treatment-seeking individuals compared to clinicians. Evidence from the broader direct-to-consumer marketing in psychiatric care suggests the potential for educating patients about evidence-based treatments to encourage them to seek care, thus increasing demand for those services from clinicians (Becker, 2015). Furthermore, there is precedent for shifts in psychiatric terminology because of poor public perceptions, rather than due to underlying changes in scientific principles. For instance, language around addiction and individuals who use substances is shifting rapidly, thanks to concerted efforts from medical societies, addiction journal editorial boards, treatment experts, and even the federal government (Botticelli & Koh, 2016). It is not a stretch to assume the same principles could be applied to market exposure therapy to both practicing clinicians and patients who may benefit. Increasing patient demand for exposure may also alleviate clinician concerns that patients will drop out or refuse exposure therapy.
It is incumbent upon the scientific community and those of us who develop, test, and implement effective interventions to present them in ways that are understandable and palatable to clinicians and patients alike. Investing work in this space is critical toward closing a particularly stubborn research to practice gap. If we truly want to realize the promise of exposure strategies to alleviate the suffering of those with anxiety, it is well worth the effort to determine how to best market exposure therapy to clinicians to motivate them to adopt this effective treatment into their practice.
Data availability
Data reported in this manuscript are available from the first author upon reasonable request.
References
Abramowitz, J. S., Deacon, B. J., & Whiteside, S. P. (2019). Exposure therapy for anxiety: Principles and practice (2nd ed.). Guilford Publications.
Alserhan, B. A., & Alserhan, Z. A. (2012). Naming businesses: names as drivers of brand value. Competitiveness Review: An International Business Journal. https://doi.org/10.1108/10595421211247169
Becker, S. J. (2015). Direct-to‐consumer marketing: A complementary approach to traditional dissemination and implementation efforts for mental health and substance abuse interventions. Clinical Psychology: Science and Practice, 22(1), 85. https://doi.org/10.1111/cpsp.12086
Becker, S. J., Helseth, S. A., Tavares, T. L., Squires, D. D., Clark, M. A., Zeithaml, V. A., & Spirito, A. (2020). User-informed marketing versus standard description to drive demand for evidence-based therapy: A randomized controlled trial. American Psychologist, 75(8), 1038. https://doi.org/10.1037/amp0000635
Becker-Haimes, E. M., Okamura, K., Wolk, C. B., Rubin, R., Evans, A. C., & Beidas, R. S. (2017a). Predictors of clinician use of exposure therapy in community mental health settings. Journal of Anxiety Disorders. https://doi.org/10.1016/j.janxdis.2017.04.002
Becker-Haimes, E. M., Franklin, M., Bodie, J., & Beidas, R. S. (2017b). Feasibility and acceptability of a toolkit to facilitate clinician use of exposure therapy for youth. Evidence-Based Practice in Child and Adolescent Mental Health, 2(3–4), 165–178. https://doi.org/10.1080/23794925.2017.1383867
Becker-Haimes, E. M., Byeon, Y. V., Frank, H. E., Williams, N. J., Kratz, H. E., & Beidas, R. S. (2020). Identifying the organizational innovation‐specific capacity needed for exposure therapy. Depression and Anxiety, 37(10), 1007–1016. https://doi.org/10.1002/da.23035
Botticelli, M. P., & Koh, H. K. (2016). Changing the language of addiction. Journal Of The American Medical Association, 316(13), 1361–1362. https://doi.org/10.1001/jama.2016.11874
Butler, R. M., & Heimberg, R. G. (2020). Exposure therapy for eating disorders: A systematic review. Clinical Psychology Review, 78, 1–12. https://doi.org/10.1016/j.cpr.2020.101851
Chorpita, B. F., Daleiden, E. L., Malik, K., Gellatly, R., Boustani, M. M., Michelson, D., & Patel, V. H. (2020). Design process and protocol description for a multi-problem mental health intervention within a stepped care approach for adolescents in India. Behaviour Research and Therapy, 133, 103698. https://doi.org/10.1016/j.brat.2020.103698
Chu, B. C., Crocco, S. T., Arnold, C. C., Brown, R., Southam-Gerow, M. A., & Weisz, J. R. (2015). Sustained implementation of cognitive-behavioral therapy for youth anxiety and depression: Long-term effects of structured training and consultation on therapist practice in the field. Professional Psychology Research and Practice, 46(1), 70–79. https://doi.org/10.1037/a0038000
Craske, M. G., Treanor, M., Conway, C. C., Zbozinek, T., & Vervliet, B. (2014). Maximizing exposure therapy: An inhibitory learning approach. Behaviour Research and Therapy, 58, 10–23. https://doi.org/10.1016/j.brat.2014.04.006
Damschroder, L. J., Aron, D. C., Keith, R. E., Kirsh, S. R., Alexander, J. A., & Lowery, J. C. (2009). Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implementation Science, 4(1), 1–15. https://doi.org/10.1186/1748-5908-4-50
Danesi, M. (2011). What’s in a brand name? A note on the onomastics of brand naming. Names, 59(3), 175–185. https://doi.org/10.1179/002777311X13082331190119
Deacon, B. J., & Farrell, N. R. (2013). Therapist barriers to the dissemination of exposure therapy. Handbook of treating variants and complications in anxiety disorders (pp. 363–373). Springer.
Dillman, D. A., Smyth, J. D., & Christian, L. M. (2014). Internet, phone, mail, and mixed-mode surveys: The tailored design method. Wiley.
Dopp, A. R., Parisi, K. E., Munson, S. A., & Lyon, A. R. (2020). Aligning implementation and user-centered design strategies to enhance the impact of health services: results from a concept mapping study. Implementation Science Communications, 1(1), 1–13. https://doi.org/10.1186/s43058-020-00020-w
Garcia-Palacios, A., Botella, C., Hoffman, H., & Fabregat, S. (2007). Comparing acceptance and refusal rates of virtual reality exposure vs. in vivo exposure by patients with specific phobias. Cyberpsychology & behavior, 10(5), 722–724.
Gagné, J. P., Puccinelli, C., Gavric, D., Milosevic, I., McCabe, R., Soreni, N. … Rowa, K. (2021). In vivo versus imaginal: Comparing therapists’ willingness to engage in both forms of exposure therapy for repugnant obsessions. Current Psychology, 1–4. https://doi.org/10.1007/s12144-021-02161-0
Haig, M. (2003). Brand Failures: The Truth About the 100 Biggest Branding Mistakes of All Time. Kogan.
Hatch, M. J., & Schultz, M. (2003). Bringing the corporation into corporate branding. European Journal of Marketing, 37(7/8), 1041–1064.
Hipol, L. J., & Deacon, B. J. (2013). Dissemination of evidence-based practices for anxiety disorders in Wyoming: A survey of practicing psychotherapists. Behavior Modification, 37(2), 170–188. https://doi.org/10.1177/0145445512458794
Hofmann, S. G., Asnaani, A., Vonk, I. J., Sawyer, A. T., & Fang, A. (2012). The efficacy of cognitive behavioral therapy: A review of meta-analyses. Cognitive Therapy and Research, 36(5), 427–440. https://doi.org/10.1007/s10608-012-9476-1
Hoge, M. A., Stuart, G. W., Morris, J. A., Huey, L. Y., Flaherty, M. T., & Paris, M. Jr. (2019). Behavioral health workforce development in the United States. Substance Abuse and Addiction: Breakthroughs in Research and Practice (pp. 433–455). IGI Global
Kagan, E. R., Frank, H. E., & Kendall, P. C. (2018). Accommodation in youths’ mental health: Evidence and issues. Current Directions in Psychological Science, 27(4), 227–231. https://doi.org/10.1177/0963721417745889
Kessler, R. C., Petukhova, M., Sampson, N. A., Zaslavsky, A. M., & Wittchen, H. U. (2012). Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. International Journal of Methods in Psychiatric Research, 21(3), 169–184. https://doi.org/10.1002/mpr.1359
Lyon, A. R., & Koerner, K. (2016). User-centered design for psychosocial intervention development and implementation. Clinical Psychology: Science and Practice, 23(2), 180. https://doi.org/10.1111/cpsp.12154
Lyon, A. R., Dopp, A. R., Brewer, S. K., Kientz, J. A., & Munson, S. A. (2020). Designing the future of children’s mental health services. Administration and Policy in Mental Health and Mental Health Services Research, 47(5), 735–751. https://doi.org/10.1007/s10488-020-01038-x
Lyon, A. R., Pullmann, M. D., Jacobson, J., Osterhage, K., Al Achkar, M., Renn, B. N., & Areán, P. A. (2021). Assessing the usability of complex psychosocial interventions: The Intervention Usability Scale. Implementation Research and Practice, 2, 2633489520987828.
Machell, K. A., Rallis, B. A., & Esposito-Smythers, C. (2016). Family environment as a moderator of the association between anxiety and suicidal ideation. Journal of Anxiety Disorders, 40, 1–7. https://doi.org/10.1016/j.janxdis.2016.03.002
Maurya, U. K., & Mishra, P. (2012). What is a brand? A perspective on brand meaning. European Journal of Business and Management, 4(3), 122–133.
Olatunji, B. O., Deacon, B. J., & Abramowitz, J. S. (2009). The cruelest cure? Ethical issues in the implementation of exposure-based treatments. Cognitive and Behavioral Practice, 16(2), 172–180. https://doi.org/10.1016/j.cbpra.2008.07.003
Ong, C. W., Clyde, J. W., Bluett, E. J., Levin, M. E., & Twohig, M. P. (2016). Dropout rates in exposure with response prevention for obsessive-compulsive disorder: What do the data really say? Journal of Anxiety Disorders, 40, 8–17. https://doi.org/10.1016/j.janxdis.2016.03.006
Proctor, E. K., Toker, E., Tabak, R., McKay, V. R., Hooley, C., & Evanoff, B. (2021). Market viability: a neglected concept in implementation science. Implementation Science, 16(1), 1–8. https://doi.org/10.1186/s13012-021-01168-2
Sammut, R., Griscti, O., & Norman, I. J. (2021). Strategies to improve response rates to web surveys: a literature review. International Journal of Nursing Studies, 104058. https://doi.org/10.1016/j.ijnurstu.2021.104058
Sareen, J., Cox, B. J., Afifi, T. O., de Graaf, R., Asmundson, G. J., Have, T., M., & Stein, M. B. (2005). Anxiety disorders and risk for suicidal ideation and suicide attempts: a population-based longitudinal study of adults. Archives of general psychiatry, 62(11), 1249–1257. https://doi.org/10.1001/archpsyc.62.11.1249
Trivasse, H., Webb, T. L., & Waller, G. (2020). A meta-analysis of the effects of training clinicians in exposure therapy on knowledge, attitudes, intentions, and behavior. Clinical Psychology Review, 101887. https://doi.org/10.1016/j.cpr.2020.101887
Tsai, Y. L., Dev, C. S., & Chintagunta, P. (2015). What’s in a brand name? Assessing the impact of rebranding in the hospitality industry. Journal of Marketing Research, 52(6), 865–878. https://doi.org/10.1509/jmr.13.0221
Voyer, B. G., Kastanakis, M. N., & Rhode, A. K. (2017). Co-creating stakeholder and brand identities: A cross-cultural consumer perspective. Journal of Business Research, 70, 399–410. https://doi.org/10.1016/j.jbusres.2016.07.010
Whiteside, S. P., Deacon, B. J., Benito, K., & Stewart, E. (2016a). Factors associated with practitioners’ use of exposure therapy for childhood anxiety disorders. Journal of Anxiety Disorders, 40, 29–36. https://doi.org/10.1016/j.janxdis.2016.04.001
Whiteside, S. P., Sattler, A., Ale, C. M., Young, B., Hillson Jensen, A., Gregg, M. S., & Geske, J. R. (2016b). The use of exposure therapy for child anxiety disorders in a medical center. Professional Psychology: Research and Practice, 47(3), 206. https://doi.org/10.1037/pro0000077
Wheeler, A. (2003). Designing Brand Identity. Wiley.
Williams, A. S., Son, S., Walsh, P., & Park, J. (2021). The influence of logo change on brand loyalty and the role of attitude toward rebranding and logo evaluation. Sport Marketing Quarterly, 30(1). https://doi.org/10.32731/smq.291.032021.06
Acknowledgements
The authors gratefully acknowledge Dr. David Mandell and Dr. Miya Barnett for their helpful comments on earlier drafts of this article. The authors also are grateful to Ms. Katherine Wislocki for her support in collecting the data presented in this article.
Funding
Dr. Stewart was supported by National Institute of Drug Abuse K23DA048167. Dr. Frank was supported by the National Institutes of Health T32MH019927.
Author information
Authors and Affiliations
Contributions
EBH and HEF initially conceptualized this manuscript and contributed to data collection. EBH wrote the initial draft and authors HEF and RES provided substantial input across several iterative revisions. All authors reviewed and approved the final submitted manuscript.
Corresponding author
Ethics declarations
All respondents provided informed consent prior to participation and were entered into a lottery to win one of ten $35 electronic gift cards as a thank you for participating. Procedures were approved by the Institutional Review Board at the University of Pennsylvania on December 22, 2020 (Protocol #844749).
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Becker-Haimes, E.M., Stewart, R.E. & Frank, H.E. It’s all in the name: why exposure therapy could benefit from a new one. Curr Psychol 42, 21641–21647 (2023). https://doi.org/10.1007/s12144-022-03286-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12144-022-03286-6